
Pain management therapy is the structured use of medical, physical, and psychological treatments aimed at reducing pain and restoring function. It is not a single treatment. It is a coordinated approach that draws on multiple disciplines to address pain from every angle. Chronic pain affects about 20% of adults, with 8% experiencing high-impact cases that limit daily activities. That scale makes understanding pain management therapy one of the most practically useful things you can do for your health right now.
What is pain management therapy and what does it actually involve?
Pain management therapy is defined in clinical practice as a multimodal treatment approach combining pharmacological, physical, and psychological strategies to reduce pain and improve quality of life. The industry standard term is "multimodal pain management," and you will hear it used by specialists, NICE guidelines, and NHS pain services alike. The goal is not simply to lower your pain score on a scale of 1–10. A pain management specialist measures success by improvements in daily activities, sleep, and mobility, not just numbers.
This distinction matters enormously. Plenty of people arrive at a pain clinic expecting a magic injection that will switch off their pain. What they find instead is a programme built around restoring what pain has taken from them: the ability to walk the dog, sleep through the night, or get back to work. Multimodal care addressing biological, psychological, and social factors consistently outperforms opioid monotherapy for long-term outcomes. That is not a minor footnote. It is the central logic behind how modern pain services are designed.

Pain therapy also sits within a clear framework of oversight. NICE guidelines in the UK set the standards for what constitutes evidence-based care, and multidisciplinary pain services are structured to deliver exactly that. Sportsinjurydublin operates on this same principle: treat the whole person, not just the symptom.
What types of pain management therapy are available?
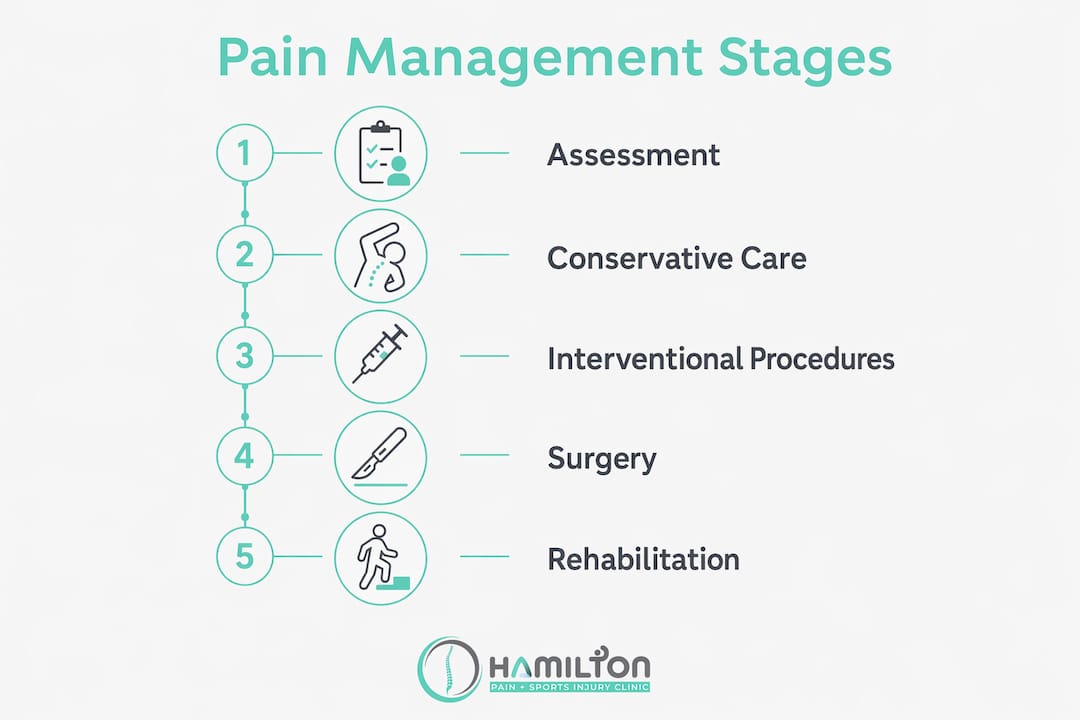
Pain management divides into three main categories: conservative care, interventional procedures, and surgery. Most people will never need surgery. The vast majority of chronic pain treatment options sit firmly in the first two categories.
Conservative therapies
Conservative care covers the broadest range of pain relief methods and is almost always the starting point. This includes:
- Medications: analgesics, anti-inflammatories, and nerve pain drugs such as gabapentinoids
- Physical therapy: exercise programmes, physiotherapy, and sports rehabilitation targeting strength and movement
- Lifestyle changes: sleep hygiene, weight management, pacing strategies, and stress reduction
- Complementary therapies: deep tissue massage, dry needling, and shockwave therapy
Interventional procedures
Interventional pain management uses minimally invasive procedures that target pain's anatomical source with fewer systemic effects than oral medications. Examples include nerve blocks, epidural steroid injections, and radiofrequency ablation. These are typically outpatient procedures and form part of a broader multimodal plan rather than a standalone fix.
| Type of therapy | Typical duration | Primary goal | Best suited for |
|---|---|---|---|
| Physical therapy | 6–12 weeks | Restore movement and strength | Musculoskeletal and post-injury pain |
| CBT / psychological therapy | 8–12 weeks | Reduce disability and distress | Chronic pain with emotional impact |
| Nerve blocks / injections | Single session, repeated | Targeted short-term relief | Localised nerve or joint pain |
| Pain Management Programme | 8 weeks | Self-management and function | Persistent, complex chronic pain |
| Medications | Ongoing with annual review | Symptom control | Moderate to severe pain of all types |
Pro Tip: Ask your clinician which category your treatment falls into. If you are only being offered one type, that is worth questioning. The evidence strongly favours combining approaches.
How does a pain management programme work?
A Pain Management Programme (PMP) is a structured group-based treatment that typically runs for 8 weeks, covering education, mindfulness, pacing, and goal setting. It is not a passive experience. You are expected to show up, engage, and practise what you learn between sessions.
A typical PMP covers these core areas:
- Pain physiology education: understanding why your nervous system produces pain and why that does not always mean tissue damage
- Mindfulness and stress management: practical techniques to reduce the emotional amplification of pain signals
- Pacing: learning to balance activity and rest so you avoid the boom-and-bust cycle that most chronic pain sufferers know all too well
- Goal setting: identifying what functional improvements matter most to you personally
- Cognitive Behavioural Therapy (CBT): retraining thought patterns that increase pain-related disability
The psychological foundations of a PMP are particularly important. CBT targets disability and emotional distress rather than aiming to eliminate pain directly. It is a gradual process that retrains the brain over weeks. Acceptance and Commitment Therapy (ACT) works alongside CBT, helping people build a meaningful life even when some pain persists.
Annual medication reviews are recommended within PMPs because long-term analgesic benefits are limited and safety monitoring is non-negotiable. This is not the programme telling you to suffer without medication. It is the programme being honest about what medication can and cannot do over the long term.
Pro Tip: The people who get the most from a PMP are the ones who treat it like a part-time job for 8 weeks. Do the homework. Practise the mindfulness. Track your activity. The results compound.
What role do non-pharmacological strategies play?
Non-pharmacological strategies are not the "alternative" option. They are the first-line option. Exercise is the preferred non-pharmacological treatment per NICE guidelines, and the evidence behind it is substantial. Movement reduces pain sensitivity, improves mood, builds resilience, and restores the functional capacity that chronic pain erodes.
Physiotherapy and occupational therapy both play central roles here. The key distinction is that modern physiotherapy for chronic pain emphasises progressive activity rather than passive treatments. Lying on a table having your muscles massaged feels nice, but it does not retrain your nervous system. Graded exercise does. Physical therapy focused on progressive activity is consistently more effective for long-term outcomes than passive measures alone.
Psychological therapies sit alongside exercise as a genuine first-line treatment, not an afterthought. CBT improves coping, builds emotional resilience, and changes the way the brain processes pain signals over time. For people with chronic back pain or persistent joint pain, combining exercise with psychological support produces better results than either approach alone.
Other non-pharmacological tools worth knowing about:
- Dry needling: targets trigger points and myofascial pain with precision
- Shockwave therapy: stimulates tissue repair in tendons and chronic soft tissue conditions
- Mindfulness-based stress reduction (MBSR): reduces the emotional load of persistent pain
- Sleep optimisation: poor sleep amplifies pain; addressing it directly improves outcomes
Pro Tip: Set one enjoyable physical goal each week, not a pain-reduction goal. "Walk to the park and back" beats "reduce pain by 20%" every time. Enjoyable goals get done. Pain-reduction goals create anxiety.
How are medications and interventional treatments integrated?
Medications remain part of most chronic pain treatment plans, but their role has shifted considerably. The main classes used are analgesics (paracetamol, NSAIDs), nerve pain drugs (gabapentin, pregabalin, amitriptyline), and in some cases, opioids for short-term or cancer-related pain. The evidence for long-term opioid use in non-cancer chronic pain is weak. That is not a controversial opinion. It is the clinical consensus reflected in NICE guidance.
Interventional procedures fill the gap between medication and surgery. Minimally invasive interventional techniques target pain's anatomical source directly, with fewer systemic side effects than oral drugs. Common options include:
- Nerve blocks: local anaesthetic injected near a specific nerve to interrupt pain signals
- Epidural steroid injections: reduce inflammation around spinal nerve roots, useful for disc-related pain
- Radiofrequency ablation: uses heat to disrupt nerve conduction, providing longer-lasting relief in facet joint pain
- Trigger point injections: address localised muscle pain that does not respond to manual therapy
These procedures work best as part of a multimodal plan. An epidural injection that gives you a six-week window of reduced pain is most valuable when you use that window to build strength and engage with rehabilitation. The injection alone rarely changes the long-term picture.
| Treatment | Typical indication | Duration of effect |
|---|---|---|
| NSAIDs | Inflammatory and musculoskeletal pain | Short-term, ongoing |
| Gabapentinoids | Neuropathic and nerve pain | Ongoing with review |
| Epidural steroid injection | Disc herniation, spinal stenosis | Weeks to months |
| Radiofrequency ablation | Facet joint pain | 6–18 months |
| Nerve block | Localised nerve pain | Variable |
How can you prepare for pain management therapy?
Preparation makes a real difference to how much you get from treatment. The single most useful thing you can do before your first appointment is keep a pain diary for two weeks. Comprehensive symptom history including psychological and social factors improves treatment tailoring significantly. A diary gives your clinician far more to work with than a verbal summary delivered under pressure in a 20-minute appointment.
Beyond the diary, here is what actually helps:
- Write down how pain affects your sleep, work, relationships, and mood, not just where it hurts
- Note what makes pain better or worse, including activity, rest, stress, and weather
- List all current medications, including supplements and over-the-counter drugs
- Bring a list of treatments you have already tried and what happened
- Come with realistic expectations: the goal is better function, not zero pain
Active engagement is a critical predictor of successful long-term pain management. Patients who treat therapy as something done to them, rather than something they participate in, consistently get worse results. Success requires sustained effort over weeks to months. That is not a warning. It is genuinely good news, because it means the outcome is largely in your hands.
Pro Tip: Tell your clinician what you want to be able to do again. "I want to play with my grandchildren without needing to sit down every five minutes" is more useful clinical information than "I want less pain." Functional goals drive better treatment plans.
Key takeaways
Pain management therapy works best when it combines physical, psychological, and pharmacological approaches rather than relying on any single treatment.
| Point | Details |
|---|---|
| Multimodal care is the standard | Combining physical, psychological, and medical treatments consistently outperforms single-method approaches. |
| Success is measured by function | Specialists track improvements in sleep, mobility, and daily activities, not just pain scores. |
| Exercise is first-line treatment | NICE guidelines recommend exercise as the primary non-pharmacological therapy for chronic pain. |
| PMPs run for 8 weeks in groups | Pain Management Programmes combine CBT, mindfulness, pacing, and education over a structured period. |
| Active engagement drives results | Patients who participate fully and consistently get significantly better long-term outcomes. |
What I have learned from working with people in pain
Here is something that took me a while to accept: most people who come in for pain management therapy are not looking for information. They are looking for permission. Permission to stop pushing through, to ask for help, and to take their pain seriously as a medical problem rather than a personal failing.
The biggest misconception I encounter is that effective therapy means eliminating pain entirely. It rarely does, and chasing that goal often makes things worse. The people who do best are the ones who shift their focus from "how do I get rid of this?" to "how do I get my life back?" That reframe is not resignation. It is strategy.
Pain is genuinely complex. It is biological, psychological, and social all at once. A sprained ankle heals in weeks. Chronic pain persists because the nervous system has learned to produce it, and unlearning that takes time, consistency, and a willingness to engage with approaches that feel counterintuitive (yes, I mean exercising when everything hurts). The biopsychosocial model is not a soft alternative to "real" medicine. It is the most evidence-backed framework we have.
The empowering part, and I mean this sincerely, is that self-management works. Education, pacing, and psychological tools give you genuine control over your experience of pain. That is not nothing. That is everything.
— Mark
Pain management support available in Dublin
Living with chronic pain and not knowing where to start is genuinely frustrating. Sportsinjurydublin at Hamilton Pain and Sports Injury Clinic in Glasnevin offers personalised treatment plans that combine physical therapy, rehabilitation, and advanced techniques tailored to your specific condition and lifestyle.
Whether you are dealing with persistent back pain, joint issues, or post-injury recovery, the clinic's approach goes well beyond generic protocols. Every plan is built around what you actually need to get back to doing. You can book a consultation and get a clear picture of which pain management strategies are right for you, without the guesswork of trying to piece it together alone.
FAQ
What is the difference between acute and chronic pain therapy?
Acute pain therapy targets short-term injury or post-surgical pain and typically resolves within three months. Chronic pain therapy addresses persistent pain lasting beyond three months and requires a multimodal, long-term approach.
Does pain management therapy include medication?
Yes, medications such as analgesics, anti-inflammatories, and nerve pain drugs are part of many pain management plans. Annual medication reviews are recommended to monitor safety and reassess long-term benefit.
How long does pain management therapy take to work?
Most structured programmes run for 8–12 weeks before measurable functional improvements appear. CBT and exercise-based approaches produce gradual changes, with sustained effort over months delivering the best outcomes.
Is CBT really effective for physical pain?
CBT does not remove pain directly but reduces the disability and emotional distress associated with it. Over time, it produces genuine changes in how the brain processes pain signals, making it one of the most evidence-backed tools in chronic pain management.
Can I access pain management therapy without a GP referral?
Access routes vary. Some services require a GP referral, particularly NHS pain clinics. Private clinics such as Sportsinjurydublin can typically be accessed directly without a referral, allowing faster entry into treatment.